|
Altered States of Consciousness New Theories on the Peak Experience and Mechanisms of Female Orgasm and Expanded Sexual Response |
|
|
|
|
|
ABSTRACT |
|
|
Although there are many forms of female orgasms described in the literature, there are still debates about the female orgasmic response and no unified theory to explain those orgasmic reflexes and sexual responses have been proposed. Also, there are inconsistent reports and comments about the ‘vaginal versus clitoral orgasm controversy’. Recently, a novel form of female orgasms has been coined as “Expanded Sexual Response” (ESR), and defined as: “being able to attain long lasting and/or prolonged and/or multiple and/or sustained orgasms and/or status orgasmus that lasted longer and more intense than the classical orgasm patterns defined in the literature”. Expanded orgasms induce a different state of consciousness, or “orgasmic consciousness”, whereas many forms of altered states of consciousness (ASC) can be observed. There are lots of reports, coming from the data accumulated during last decades on the female orgasm and orgasmic consciousness, which confirms the fact that “clitoral and vaginal orgasms are two separate entities”, while their unification may induce a stronger and intense form of female orgasm, coined as “blended orgasm”. As we have hypothesized in our other publications, at least six orgasmic reflex pathways may take part in the development of single or multiple clitoral, vaginal, blended orgasms, and expanded, enhanced, prolonged ESR orgasms. Pudental, pelvic, hypogastric and vagus nerves play major roles in the development of single or ESR orgasms, as well as at least two oxytocin pathways may contribute to it. In blended, ESR orgasms and/or status orgasmus, more than one ‘orgasm reflex arch pathways’ may trigger the orgasm at the same time, while other pathways play a supplementary role. We have investigated the ESR phenomenon using a specific ESR-Scale in a series of surveys among ESR-women, compared to the control groups and defined the main characteristics of ESR phenomenon in the human female. ESR women seem to have higher libido, higher masturbation frequency, more erotic fantasies, stronger and more intense, prolonged orgasms or expanded orgasms (EO); while they experience multiple clitoral, vaginal and blended orgasms separately. Also ESR women are more aware of their bodies and their deep vaginal erogenous zones (DVZ), which comprises inner clitoris, G-Spot, A-Spot, O-Spot, PC-Muscles and Cervix. “Four nerve-six pathway theory of female orgasm” and oxytocinergic system may seem to explain ESR phenomenon. |
|
|
|
|
|
|
|
|
|
|
Female orgasm and female orgasmic ‘peak experiences’ have been well documented in the ancient historical literature (Vatsyayana, 1883; Chang 1977, 1983; Wu, 1996; Schwartz, 1999; Chia 2002, 2005; Mumford, 2005; Michaels 2008). Eastern cultures had tried to discover the limits and extents of female orgasmic response for centuries (Wu, 1996; Chang, 1977, 1983). It was Sigmund Freud who first pronounced the existence of different kinds of female orgasms; according to his theory, mature female orgasms were “vaginal orgasms”, that occurred during coitus; however, long after his theories, Masters and Johnson’s clitoris oriented orgasm theory became valid and “clitoral orgasm theory” established the basis of sex therapy for decades (Masters & Johnson, 1966, 1970, 1995). According to Masters and Johnson, clitoris was the main focus that triggered female orgasm, as they rejected the ‘vaginal orgasm theory’ (Masters & Johnson, 1966), since vaginal orgasms were not observed frequently in their laboratory experiments; they explained vaginal orgasms as a variation of “clitoral orgasms”, whereas glans clitoris was the target of orgasmic response in both forms of orgasms. Some surveys, pointed out that a “hypothetical vaginal orgasm” existed in some women; according to Hite Report (Hite, 1974) and Cosmo Report (Wolfe, 1983) only one third of American women were able to attain “vaginal orgasms”.
After the book “G-Spot” was published in 1982, a new debate was started about the “clitoral versus vaginal orgasms” which still continues (Ladas, 1982). Ladas et al. hypothesized that vaginal orgasms originated by means of the stimulation of G-Spot via pelvic nerve, which was a rudimentary embryologic prostatic structure in the frontal wall of vagina at the mid length of urethra (Ladas, 1982). Recently, other intra-vaginal erogenous zones have been proposed to be discovered that may take part in the mechanisms of female orgasms (Morris, 2004; Sayin 2012 a-b-c). Also Komisaruk et al. and Sayin et al. (Komisaruk, 2006; Sayin, 2010, 2011 a-b-c, 2012 a-b-c) have reported that female orgasm can be triggered by means of the stimulation of other erogenous zones via different neural pathways, while “the brain” and the psychology of the woman played the major role. According to the novel accumulating data, glans clitoris was responsible of the ‘clitoral orgasms’ via a reflex pathway originating from pudental nerve and sacral plexus, while other vaginal erogenous zones, coined as “deep vaginal erogenous zones” (DVZ) were responsible of ‘vaginal orgasms’, via other orgasm reflex pathways, such as pelvic nerve-sacral plexus, hypogastric nerve-pelvic plexus and vagus nerve-brain (Komisaruk, 2003, 2004, 2005, 2006; Sayin, 2010, 2011a-b-c, 2012a-b-c, 2013). Also the term of “blended orgasm” had been defined by Ladas et al. (Ladas, 1983) and Sayin et al. (Sayin, 1993, 2010, 2011c, 2012a-b). “Four nerve theory of female orgasmic response” was hypothesized to explain the mechanisms of single, multiple and extreme prolonged orgasms or ESR in the human female (Komisaruk, 2006; Sayin, 2011 c, 2012 a-b, 2013).
Lately, a novel phenomenon was defined and coined as “expanded orgasm” (EO) and “expanded sexual response” (ESR) in a minority of women (Taylor, 2000, 2002; Sayin, 2010, 2011c, 2012a). ESR was defined as, “being able to attain long lasting and/or prolonged and/or multiple and/or sustained orgasms and/or status orgasmus that lasted longer and more intense than the classical orgasm patterns defined in the literature” (Sayin, 2010, 2011a-b-c, 2012a, 2013). The duration of EO and ESR varied from woman to woman, lasting starting from a couple minutes to hours (Schwartz, 1999; Taylor, 2000, 2002; Sayin, 2010, 2012a, 2013). In the literature the highest number of orgasms in a woman recorded by Dr. William Hartman and Marilyn Fithian was reported to be 134 per hour (Sayin, 2010, 2012a).
Although defined recently, ESR and EO were not new phenomenon, but peak experiences of female orgasmic consciousness defined by different cultures centuries ago (Chang 1977, 1983; Wu, 1996; Schwartz, 1999; Chia 2002, 2005), while ESR may induce altered states of consciousness (ASC) and peak experiences in some women (Taylor, 2000, 2002; King, 2010; Sayin 2010, 2011c, 2012a, 2013).
This article briefly discusses some novel findings, hypotheses and theories on the mechanisms of female orgasms, ESR and peak experiences of consciousness occurring during the enhanced and prolonged female orgasms.
The Nature of Female Orgasm
Female orgasm is a neuro-psychological response and peak experience that results from the accumulated sexual tension, sexual stimulation, arousal and internal sexual build up, which is accompanied by neural and psychological discharge. As Masters & Johnson, Hartman & Fithian investigated in the laboratory conditions, female orgasmic response is complemented by the contraction of some voluntary and involuntary musculature, such as vulva, vagina, uterus, pelvic floor muscles (PFM), some of body muscles (leg, abdomen, pelvic muscles etc.) (Masters & Johnson, 1966; Sayin 2010, 2012a).
Some researchers have described female orgasm as (from, Mah & Binik, 2001):
· Neurohormonal reaction of smooth muscle organs and contraction of homologues of ejaculatory muscles (Campell and Peterson, 1953).
· Spastic vaginal contractions occurring at highest tension levels (Glann and Kaplan, 1968).
· Reflexive sensory-motor response involving genitopelvic contractions (Kaplan, 1974).
· Reflexive sensory-motor response to sexual stimulation (Kline-Graber and Graber, 1975).
· Release of vaso-concentration and myotonia from sexual stimulation (Masters & Johnson, 1966).
· Altered states of consciousness (Davidson and Davidson, 1980).
· Involuntary reflex action accompanied by uterine / vaginal contractions (Reubens, 1982).
· Psychic phenomenon, a sensation (cerebral neuronal discharge) elicited by the accumulative effect on certain brain structures of appropriate stimuli originated in the peripheral erogenous zones (Alzate, 1985).
· Complex experiences of genital changes, changes in skeletal muscle tone/semi-voluntary movements, cardiovascular / respiratory changes (Bancroft, 1989).
· Sudden, intense sensation just prior to genitopelvic contractions (Hite, 1976).
· Acme of sexual pleasure with rhythmic convulsions of the body of perineal/reproductive organs, cardiovascular and respiratory changes, release of sexual tension (Schiavi and Segraves, 1995).
· Orgastic potency; capacity to surrender to flow of biological energy; capacity to discharge the dammed-up sexual excitation through involuntary, pleasurable convulsions of the body (Reich, 1973).
When we look at the nature of female orgasm, although there are similar patterns to male orgasm, it seems to be very different than male ejaculation depending upon the woman experiencing it. In a classical single female orgasm, there seems to be different patterns contributing the bodily changes:
· Whole body changes: tachycardia, elevated blood pressure, hyperventilation, sweating, extension of some muscle groups (e.g. legs and feet), muscle tension, ‘sex flush’, vasodilatation at the cutaneous arterioles and increased venous blood pounding etc.
· Genito-Pelvic changes: erection of clitoral complex and glans clitoris, enlargement of G-Spot area and urethral sponge, lubrication, involuntary contraction of vagina, uterus and cervix, voluntary-involuntary contraction of pelvic floor muscles (PC-muscles), involuntary contraction of anal sphincter etc.
· Psychological changes: Relief of tension, discharge feeling, decrease of anxiety, happiness, euphoria, relaxation, fulfillment, subjective feeling of getting rid of electrical and muscle tension, altered states of consciousness (ASC) etc.
As measured by Masters & Johnson, the contraction duration of genito-pelvic area occurs at 0.8 second intervals (Masters & Johnson, 1966). Although males have a refractory period after one orgasm, or ejaculation, to become erect again, it has been well documented that females have the capacity to continue having multiple climaxes if they are stimulated continuously and properly (Schwartz 1999; Bodansky, 2000; Taylor 2000; Komisaruk, 2006; Sayin 2010, 2012a, 2013). As described by Masters & Johnson, some women can attain an orgasmic state which may last for 43 seconds, coined as status orgasmus (Masters & Johnson, 1966). In some women who have developed ESR; EO, multiple orgasms and status orgasmus can vary in duration and in number of minor orgasms they contain in the train of orgasmic pattern. Lately, such prolonged orgasms and the methods how to attain them have been published in many books and articles (Rhodes, 1991; Schwartz 1999; Bodansky, 2000; Taylor 2000, 2002; Komisaruk, 2006; Sayin 2010, 2011a-c, 2012a, 2013; Deadone, 2011). We have defined status orgasmus as (Sayin, 2010, 2011c, 2012a-b, 2013);
Status orgasmus is the continuous form of blended orgasms and/or clitoral/vaginal orgasms that last for starting from 1 minute to 10-15 minutes (or more). During status orgasmus a continuous orgasmic state is experienced and very few women are believed to achieve status orgasmus state. Status orgasmus can be seen in vaginal and clitoral orgasms, however mostly it is seen as an expanded/extended form of blended orgasms, in which both clitoral and vaginal orgasm reflexes are triggered at the same time. Similar orgasmic states and full body orgasms are also defined in Tantric literature. The duration may change from woman to woman. Status orgasmus was first defined by Masters & Johnson as lasting for 43 seconds in a woman in 1966. Today it is estimated that status orgasmus continues for 1 to 2 minutes, while it may last for 10 to 15 minutes, a prolonged and extended orgasmic state which ends by a giant orgasm (Big-O) that gives a great relief and satisfaction at the end. In most of the status orgasmus experiences there is usually a refractory period of 10 to 15 minutes. The number of minor orgasms in a status orgasmus may exceed from 5-10 to 20-30 (some women claim that this quantity goes up to around 50). In status orgasmus it is thought that any combination of pudental, pelvic, hypogastric and vagal nerves mediate the triggering mechanism at the same time.
As a novel phenomenon “ESR orgasms and EO” seem to be different in many ways from the classical single orgasms, as defined by Masters & Johnson and Kaplan (See Fig-1; Masters & Johnson, 1966; Kaplan, 1981; Rhodes, 1991; Schwartz, 1999; Taylor, 2000, 2002; Diadone, 2011; Sayin, 2010, 2011c, 2012a-b, 2013):
· The duration of single orgasms in the orgasmic train may increase.
· The duration of the whole orgasmic experience may increase, such as lasting for tens of minutes to a couple of hours.
· The intensity of the individual minor orgasms generally increases along with the length of the orgasmic train.
· The number of minor orgasms in the orgasmic train may be beyond the normal and average orgasmic pattern, such as exceeding 20-30 orgasms in tens of minutes.
· The pleasure taken and sexual relief is reported to be much more compared to single or a couple of multiple orgasms.
· Without a refractory period, a new orgasmic state commences after each orgasm, without passing to a resolution phase, while orgasmic consciousness state is maintained for a long time (e.g. from a couple of minutes to tens of minutes or hours)
· Although there may be some forms of ASCs in some single orgasms of some women, most of the ESR and EO orgasms are accompanied with ASCs, whereas time perception, space-time continuum may be altered deeply. We had reported 72 different states of mind in our former publication (Sayin, 2011c).
· As reported by many ESR women, ESR orgasms seem to have anxiolytic, anti-depressive, euphoric, myorelaxant, sedating, analgesic, acute and short acting hallucinogenic effects which made us to adopt a humorous novel slogan: “Don’t use drugs! Use Expanded Orgasms!” (Sayin 2011c; Sayin 2012a-d).
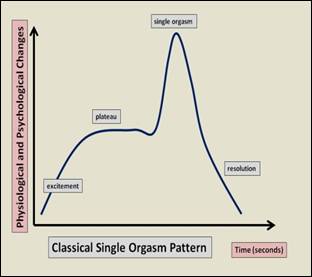
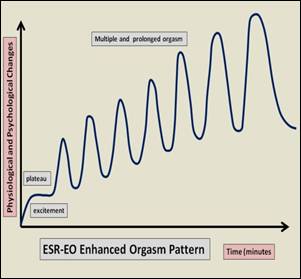
Figure 1. Left: Classical female orgasm pattern, defined in the classical medical literature, Right: Enhanced and expanded orgasm pattern in ESR and EO, as defined in various resources recently.
Clitoral versus Vaginal Orgasms
Clitoral stimulation is the main source of sensory input for triggering a female orgasm; glans clitoris, which contains nearly 8000 nerve endings, can trigger an orgasm when stimulated manually, by friction, vibration, cunnilingus, or indirect penile trust stimulation in most of the women (Masters & Johnson, 1966; Kline-Graber, 1975; Kaplan, 1981). Orgasms attained through clitoral stimulation have been reported to be more localized, sharp, bursting, short lasting, superficial, confined only to the pubic area; while coital vaginal orgasms have been described as more diffuse, “whole body”, radiating, psychologically more satisfying, lasting longer, having more tendency to turn into multiple orgasms (Fisher, 1973; Hite, 1976; Kline-Graber, 1975; Mah, 2001; Komisaruk, 2006; Sayin, 1993, 2010, 2012a, 2013).
Singer gives another typology of female orgasm (Singer, 1973): 1) Vulva orgasm: identified by orgasmic platform contractions and induced by coital or non-coital activity. 2) Uterine orgasm: identified by some physiological parameters such as apnea and lack of orgasmic-platform contractions and induced by cervical stimulation from deep coital trusting. 3) Blended: Having the elements of both, unified. Ladas et al. also mentioned about blended type of orgasms (Ladas, 1982). Ladas hypothesized that G-Spot was responsible for the triggering mechanisms of vaginal orgasms, while vaginal orgasms were mediated through a reflex arch through sacral plexus via pelvic nerve; clitoral orgasms were also mediated through a similar pathway via pudental nerve. According to the hypothesis defended in the book “G-Spot”, blended orgasms were the unifying of two types of orgasms, vulva-uterine orgasms, which were mediated through pudental, pelvic and hypogastric nerves (Ladas, 2005-1982).
Our extensive survey results on female sexuality (Kadınca Report-1993; Hülya Report-2003; İstanbul Report-2013, which is still continuing) among nearly 2500 women since 1991, have pointed out that, clitoral orgasms and vaginal orgasms are definitely two distinct phenomenon (Kocatürk, 2012; Sayin, 2010, 2011d, 2012a).
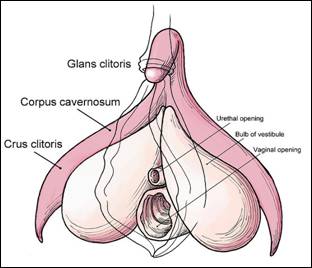
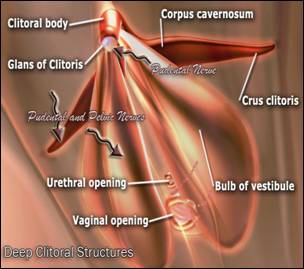
Figure 2. Deep Clitoral Structures and the Inner Clitoral Complex (left). Glans clitoris is innervated by pudental nerve, while other structures are innervated by both pudental and pelvic nerves (right).
Masters & Johnson argue about the possibility of indirect clitoral stimulation during coitus, thus according to them, the hood of clitoris inducing a friction to the glans builds up an indirect clitoral orgasm. The literature and our studies have enough data to dispute such a phenomenon. Let’s clear out the existence of a separate “vaginal orgasm”:
1) The clitoral hood cannot move directly enough to stimulate the glans during coitus. If some deep erectile structures of clitoris, such as bulbus or crus, are stimulated as well, this sensory input will not be carried by pudental nerve, because most of the deep structures of clitoral complex are innervated by pelvic nerve, which may cause another type of “clitoris-pelvic orgasm”, which is not exactly the same as “glans-pudental nerve orgasm”.
2) Most of the descriptions of each type of orgasms in the literature are very different in terms of their physiological, neuropharmacological and psychological effects (Campell, 1953; Fisher, 1973-77; Hite, 1976; Taylor, 2000, 2002; Ladas, 1981; Komisaruk, 2006; King, 2010; Sayin, 1993, 2010, 2012a). For instance, orgasms triggered by coitus induce 4 times fold prolactin release in the female brain compared to manual clitoral orgasms, which is proposed to be a measure of satiety (Brody, 2006).
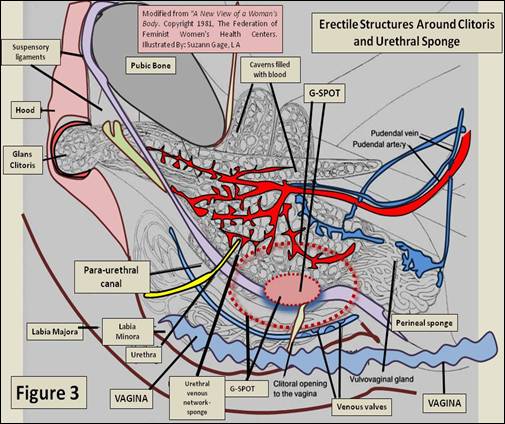
Figure 3. The venous network system surrounding the clitoral structures is depicted. Urethral sponge, deep clitoral structures, G-Spot are interconnected. Glans clitoris is innervated by pudental nerve, while most of these structures and G-Spot are innervated by pelvic nerve and some portions partially by pudental nerve.
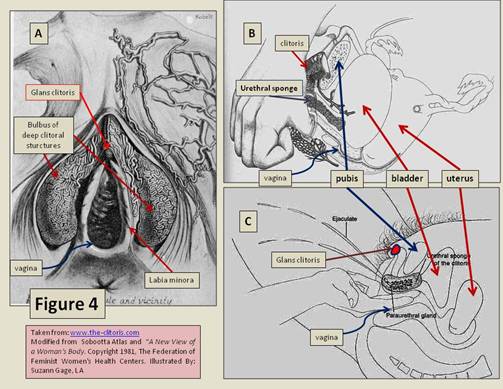
Figure 4. A) The venous blood supply of bulbus part of clitoral complex is depicted. B-C) The stimulation of urethral sponge and G-Spot area and the female ejaculation, which is observed in a minority of women, is shown.
3) It has been reported that the women who are aware of their G-Spots and who have responding-pleasurable G-Spots, are more likely to attain coital vaginal orgasms (Ladas, 1981; Sayin, 2010, 2012a-c; Hooper, 2008)
4) There appears to be other deep vaginal erogenous zones (DVZs) in some sexually hyper active and responsive women, other than clitoris and G-Spot, as reported recently (see figure-5 and below; Morris, 2004; Sayin, 2012a-b-c). Those zones are more prominent in women with ESR and high sexual responsiveness, compared to none-ESR (NESR) women or average women. Nearly 99 % of ESR women were able to attain vaginal-coital orgasms (Sayin 2011b, 2012a-b-c). Those areas are innervated by pelvic nerve and partially by hypogastric nerve, similar to G-Spot, which induce a separate orgasm reflex arch pathway; thus a very different physiological orgasmic response builds up.
5) Our preliminary studies by means of the electrical and vibration stimulation of DVZ seem to trigger orgasm patterns alone, without the stimulation of glans clitoris (unpublished data). Similar interesting data comes out of the research group of Komisaruk; stimulation of cervix alone induced orgasmic behavior in women who were hemiplegic, having no connection of nervous input from glans via pudental nerve and from vagina via pelvic nerve (Komisaruk, 2003, 2004, 2005, 2006); this is also a proof that orgasm reflexes can be triggered from the brain without the existence of input through glans clitoris.
6) In some women, undergone clitoridectomy, some coital orgasms have been reported (Sayin, 2010; Escapa, 1989), which shows that without the existence of glans clitoris, orgasms may build up by some other mechanisms, while inner clitoral complex may have some contributions to those kind of orgasms, however they are unlikely to trigger an orgasm by the stimulation of bulbus or crus of clitoris alone; there should be other triggering neural pathways and mechanisms that play major roles in the development of “orgasms without clitoris”.
7) After the definition of novel “four nerve and six pathway theory of female orgasm” (see below), it was realized that at least six different pathway-mediated orgasm reflex arches, some of which may contribute to build up “vaginal orgasms” originating from direct stimulation of DVZ, may exist! (Komisaruk, 2006; Sayin, 2011c, 2012a-b)
8) Our preliminary research and other accumulating data also showed that some specifically designed electronic dildo shaped vibrators that have a rotational and vibrating property at the tip may induce orgasms of vaginal origin (unpublished data), which may also show that stimulation of PC-muscles, O-Spot, A-Spot and Cervix may trigger vaginal orgasms in some women. Near to these findings, electrical stimulation of cervix and DVZs by a TENS unit (trans-cutaneous-electrical-nerve-stimulation unit) may induce similar vaginal orgasms (unpublished data).
9) Recently, “Brain Orgasms” without the stimulation of any genital erogenous zones have been reported (Komisaruk, 2005, 2006; Sayin, 2012a-b). If brain orgasms can exist, than we should investigate many other pathway systems and mechanisms, such as the “oxytocin pathway”, other than focusing only on the ‘glans clitoris’!
If there are separate vaginal orgasms mediated by some different neural pathways other than ‘clitoral orgasm pathway and arch’, and then there should be “blended orgasms”, as well, which may occur when both of those pathways that mediate clitoral and vaginal orgasms are activated at the same time. Our survey data on female sexuality and our researches and surveys on ESR, have revealed that such stronger, longer, more intense orgasm patterns also exist, as first described by Singer and Ladas (Singer, 1973; Ladas, 1982; Sayin, 2011a-b-c, 2012a-b-c-d, 2013; Kocatürk, 2012)
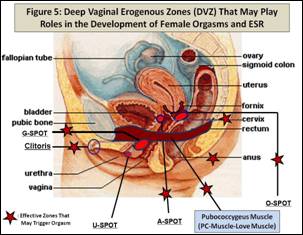
Figure 5. Deep Vaginal Erogenous Zones (DVZs) include G-Spot, inner clitoral structures of the clitoral complex, A-Spot, O-Spot, Cervix, Pelvic Floor Muscles (PC-Muscle), which have been proposed to be functional in some of the ESR-high orgasmic women to trigger different forms of orgasm patterns. The frequencies of occurrences of these areas have not yet been investigated extensively and in detail. The areas with stars are likely to trigger orgasms in a small group of women. U-Spot, although proposed by Morris in 2004, have not yet been identified in the literature and in our surveys. It has been reported that female orgasms can be mediated and triggered by various forms of stimulation of glans clitoris, inner clitoris of clitoral complex, G-Spot, A-Spot, O-Spot, Anus, Cervix, PFM, Nipples, Ear Lobes, and the brain.
Deep Vaginal Erogenous Zones (DVZ)
Recently, other erogenous zones in the deep structures of pelvic area and vagina have been described (Morris, 2004; Sayin, 2011c, 2012a-b-c, 2013). We have investigated the possible existence of such areas in our surveys and other research projects; we have come across the description of such sensitive areas that may contribute to the development of female orgasm in some women (Sayin, 2011c, 2012a-b-c, 2013). The descriptions of DVZs and occurrence frequency of the awareness of DVZs in some women, particularly with ESR (ESR women N=35; None-ESR Control women N= 163; total group N=198), were as follows (See Figure 5):
· G-SPOT (Grafenberg’s Spot): The localization of G-spot is at the anterior vaginal wall, 2.5-4 cm inside, under the mid uretral length. In our series 63 out of 198 women (31.8 %) admitted to be aware of their G-Spots. 55 of them (27.7 %) were positive that they had experienced G-Spot orgasms. 25 of these women (45.4 %) were ESR-women.
· A-SPOT: A-Spot is at the anterior wall of vagina, 2-3.5 cm below anterior fornix, under the bladder. 21 women (10.6 %) admitted to be aware of such an erogenous zone. 13 of them (61.9 %) were ESR-women.
· O-SPOT: O-Spot is between the posterior vaginal wall and the rectum, 2-4 cm below posterior fornix. 16 women (8 %) replied that they have a sensitive area at this part of their genitalia. 12 of them (75 %) were ESR-women.
· U-SPOT: U-Spot was hypothesized to exist at the area of the urethral opening by Morris (Morris, 2004). No U-Spot has been detected in the survey.
· Cervix: Cervix is the collum (neck) of uterus. 15 women (7.5 %) replied that their cervix was sensitive and might have triggered an orgasm. 9 of them (60 %) were ESR-women.
· Pelvic Floor Muscles (PFM-PC-Muscles): PFM are the muscle network between pubis and coccyx. 24 women (12.1 %) told that activation of PFM was effective for the development of an orgasm. 12 of them (50 %) were ESR women.
Most of the ESR women admitted that they may have such erogenous zones, which may take part in the development of an orgasm, other than glans clitoris. In our preliminary study in 198 women, some of the ‘DVZ spots’ were identified by ESR (N=35) and NESR women (N=163) (Sayin, 2012a-b-c).
The Arguments and Discussions about G-Spot
The G-Spot was first described by a Dutch physician Regnier de Graaf in 1672 and then by Ernst Grafenberg in 1950, as an erogenous zone on the anterior wall of vagina that expels urethral ejaculate during an intense orgasm (Ladas, 1982; Mah, 2001). Glandular structures, Skene’s paraurethral glands, have been proposed to homologous to male prostate that stayed atrophic and rudimentary during the course of embryological development (Addegio, 1981; Belzer, 1981; Perry, 1981; Ladas, 1982; Zaviacic, 1985, 1993, 1998). Many reports and surveys and laboratory observations revealed that 40 % to 66 % of the subjects reported a sensitive and pleasurable area around 11:00-1:00 (clockwise) position of the anterior wall of vagina at the mid-length of urethra (see Figure 5) (Perry, 1981; Ladas, 1982; Davidson, 1989; Weijmar Schultz, 1989; Komisaruk, 2006; Sayin, 2010, 2012a-b-c, 2013). The laboratory studies of Addegio et al. and Zaviacic et al. also showed that biochemical analysis of female ejaculate revealed that the ejaculate was different than that of urine and female ejaculate had some similar components of prostate secretion (Addegio, 1981; Zaviacic, 1985, 1988, 1995, 1998; Ladas, 1982; Sayin, 2010, 2012a).
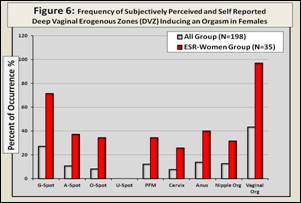
Figure 6. The investigation of DVZs among 198 women along with the survey research on ESR. The survey questionnaire had detailed descriptions and schematic figures of DVZ. The total number of 198 also includes 35 ESR women. As seen on the plot the frequency of the occurrence of DVZs’ awareness was much higher in women with ESR, who attained vaginal orgasms in nearly 99 %. Some women admitted that they experienced orgasms through the stimulation of G-Spot, A-Spot, O-Spot, Anus, PFM, Cervix, Nipples, however no one had a memory of pleasure or orgasm from the stimulation of the coordinates of an area that coincided ‘the hypothetical U-Spot’, as described by Morris in 2004.
Recently, another internet survey among 5000 women in England (2011), showed that nearly 72 % of the correspondents admitted to have G-Spots; however, 50 % of these women were able to describe the exact coordinates of G-Spot, while 35 % described it deep inside, 15 % located it elsewhere (http://www.orgasmsurvey.co.uk/pressrelease.htm). This study also confirms our hypothesis on DVZ, since 35 % of the 72 % of the study group (1260 women out of 5000 women); reveal that they have sensitive zones deep inside the vagina, assuming that DVZ was G-Spot, since they did not have any idea about the sensitivity of A-Spot, O-Spot, Cervix and PFM.
Today there are still arguments about whether the G-Spot exists or not, however, many studies and surveys showed that, although the frequency alters, from 35 to 40 % to 50-60 % of the female population confirm to have G-Spots and accept the contributions of G-Spot to the development of female orgasm.
Expanded Prolonged Orgasms (EO) and Expanded Sexual Response (ESR)
ESR is a recently defined phenomenon (Rhodes, 1991; Taylor, 2000, 2002; Armagan, 2012; Sayin, 2011a-c, 2012a-b, 2013). As ESR was defined above, the main hypothesis in ESR studies was, “Sexual response, orgasmic consciousness and experience and orgasmic pleasure can be enhanced, prolonged, and expanded in the human female”. Although a small proportion of women has attained or can attain ESR today, ESR is a learned phenomenon that can be developed in many women by training and education. To determine the main parameters and mechanisms of ESR, we have investigated the main characteristics of women who have developed ESR (Taylor, 2000, 2002; Armagan, 2012; Sayin, 2011a-b, 2012a-b-c, 2013):
1) The ESR women experienced vaginal, clitoral and blended orgasms, as described by Ladas et al. (Ladas, 1982; Taylor, 2000, 2002; Armagan, 2012; Sayin 2010, 2011a-b-c, 2012-a-b-c-d).
2) The ESR women experienced multiple orgasms in most of their sexual activities. (Schwartz, 1999; Taylor, 2000, 2002; Mamfurd, 2005; Armagan, 2012; Sayin 2010, 2011a-b-c, 2012-a-b-c-d)
3) The ESR women were able to attain long lasting and/or prolonged and/or multiple and/or sustained orgasms and/or status orgasmus that lasted longer than the classical single orgasm and/or multiple orgasm patterns defined in the literature. (Schwartz, 1999; Taylor, 2000, 2002; Sayin, 1993, 2010, 2011a-b-c, 2012a-b-c-d)
4) The ESR women claimed to have strong pelvic floor muscles (PFM) compared to NESR women. (Ladas, 1981; Britten, 1983; Sayin, 2010, 2011b, 2012a-b)
5) The libido of ESR women was very high compared to NESR women. (Armagan, 2012; Sayin, 2012a-b)
6) ESR women described a phenomenon called G-Spot orgasms. (Ladas, 1982; Taylor, 2000, 2002; Armagan, 2012; Sayin, 2010, 2011b, 2012a-b-c)
7) ESR women described sensitive erogenous zones in their genitalia other than clitoris. (Morris, 2004; Armagan, 2012; Sayin, 2012a-b-c)
8) ESR women masturbated more frequently compared to NESR women. (Armagan, 2012; Sayin, 2012a-e)
9) ESR women had erotic fantasies more frequently than the NESR women. (Armagan, 2012; Sayin, 2012a-e)
10) ESR women admitted to have a form of altered states of consciousness during some of their prolonged orgasms and/or status orgasmus (Taylor, 2000, 2002; Mah, 2001, 2002, 2005; King, 2010; Sayin, 2011c; Sayin,2012a-d).
Our preliminary findings of ESR research, which is still continuing, were presented in NACS-2011 (Oslo-Norway), IASR-2012 (Lisbon-Portugal) and NACS-2012 (Helsinki-Finland) Meetings. As a summary, some of the presented data which support above ten characteristics of ESR women were as follows (Sayin, 2012b):
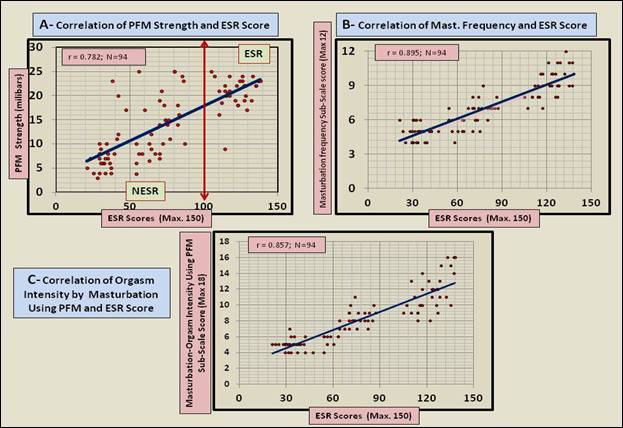
Figure 7. Partial preliminary data of ESR study, which is still continuing. A) ESR scores were directly proportional with the strength of PFM (PC-Muscles) (r=0.782, N= 94). Note that, the women who got scores above 100, were accepted as ESR-women, out of the course and statistics of the study. The women who trained PC-Muscles may become multi-orgasmic, vaginally orgasmic and training of PC-Muscles is an important factor in the development of ESR. B) Masturbation frequency is also correlated with ESR scores (r=0.895, N=94). ESR women masturbated more frequently compared to NESR-women. C) Orgasm intensity measures were also directly proportional with ESR scores. The ESR women experienced more intense, prolonged, long lasting and strong orgasms compared to NESR women (r=0.857, N= 94).
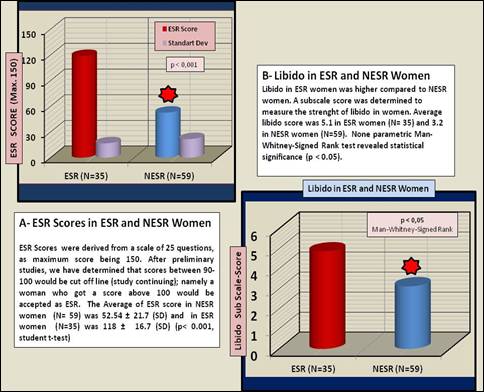
Figure 8. A) Comparison of ESR scores of ESR and NESR women. The ESR cut off line was between 90-100. We have accepted women with scores over 100, as ESR-women. B) Libido of ESR (N=35) women was much higher compared to NESR women (N=59).
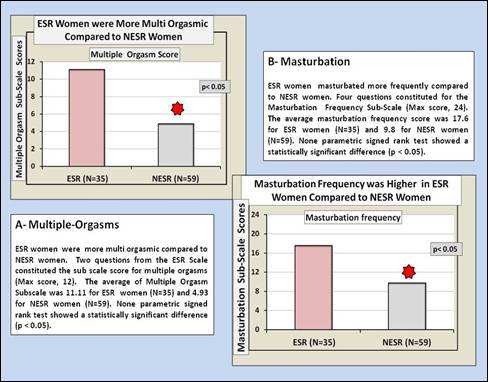
Figure 9. A) ESR women were more multi-orgasmic compared to NESR women. Multiple orgasm sub-scores of ESR women (N=35) were more than twice that of NESR women (N=59). B) Masturbation frequency sub-scores of ESR women (N=35) was nearly twice that of NESR women (N=59). ESR women masturbated more frequently than the control NESR women.
Novel Explanations of Neuro-anatomical, Neurological and Neuropharmacological Mechanisms of Single Vaginal and Clitoral Orgasms, Multiple Orgasms and ESR Orgasms
To explain the enhanced and expanded forms of female orgasmic consciousness, we had hypothesized the “Four Nerve and Six Pathway Theory of Female Orgasm” in our former publications (Sayin, 2011c, 2012a-b-f). There is a lot of data which confirms that four separate nerves carry sensory inputs from the “orgasming zones” of female genitalia or body; these are pudental, pelvic, hypogastric and vagus nerves (Ladas, 1982; Komisaruk, 2003, 2004, 2005, 2006; Sayin, 2011c, 2012a-b, 2013). The following are the possible pathways that carry sensory input to somato sensory, frontal and prefrontal cortices and the limbic system, and contribute to the formation of an “orgasm reflex” (Figure 10); some of those loci directly trigger a female orgasm, some of them may have contributions in terms of sensory input. Also there are two other oxytocinergic pathways which contribute to the formation of an orgasm of any kind (Sayin, 2011c, 2012a-f) If a single “orgasm reflex pathway”, while some other pathways having some involvement, as well, operated during the development of an orgasm; a single clitoral, vaginal or brain orgasm may occur. If many (more than one) “orgasm reflex pathways” and a combination of the following pathways are involved in the formation of an orgasm, then an EO or “ESR orgasm” may develop and orgasms may become more intense, multiple and prolonged. This is a learned and maturing phenomenon, which can be developed and improved by training and education, as many ancient Tantrists had done centuries ago (Mamford, 2005; Carellas, 2007; Sayin, 2012a).
· Glans clitoris à Pudental N. à Sacral plexus à BRAIN à Clitoral orgasm
· Parts of clitoral complex (crus, body, bulbus etc) à Pudental N. à Sacral plexus à BRAIN à Clitoral orgasm or Vaginal orgasm, or contributes
· Parts of clitoral complex (crus, body, bulbus etc) Pelvic N. à Sacral plexus à BRAIN à Vaginal orgasm, or contributes
· G-Spot à Pelvic N. à Sacral plexus à BRAIN à Vaginal orgasm; and ejaculation in some women
· Various vaginal stimulation during coitus à Pelvic N. à Sacral plexus à BRAIN à Vaginal orgasm
· A-Spot à Pelvic N. (possibly partially hypogastric N) à Sacral plexus (+ partially Pelvic plexus) à BRAIN à Vaginal orgasm, or contributes to Vaginal orgasm or ESR orgasm
· O-Spot à Pelvic N. (possibly partially hypogastric N) Sacral plexus (+ partially Pelvic plexus) à BRAIN à contributes to Vaginal orgasm, Anal orgasm or ESR orgasm
· PFM (PC-Muscle) à Pelvic N. (possibly partially hypogastric N) Sacral plexus (+ partially Pelvic plexus)à BRAIN à Vaginal orgasm, or contributes to Vaginal orgasm or ESR orgasm
· Cervix à Partially Pelvic N. + Mostly Hypogastric N. à Pelvic Plexus (+ partially sacral plexus)à BRAIN à Vaginal orgasm, or contributes to Vaginal orgasm or ESR orgasm
· Cervix à Vagus N. à BRAIN à Vaginal orgasm, or contributes to Vaginal orgasm or ESR orgasm
· Uterus à Hypogastric N. + Vagus N. à Pelvic Plexus + BRAIN à contributes to Vaginal orgasm or ESR orgasm
· Anus + Rectum à Infra Anal N. + Pudental N. + Pelvic N. + Anal sphincter nerves à Sacral Plexus à (BRAIN) à Anal orgasm (O-Spot stimulation contributes to anal orgasms)
· Nipples à Intercostal N. à Pituitary – Oxytocin Pathway à BRAINàNipple orgasm; or contributes to Clitoral orgasm, Vaginal orgasm or ESR orgasm
· BRAIN-imagination-fantasy-sexual images à Pituitary – Oxytocin Pathway à BRAINà Brain orgasm or contributes to all kind of orgasms
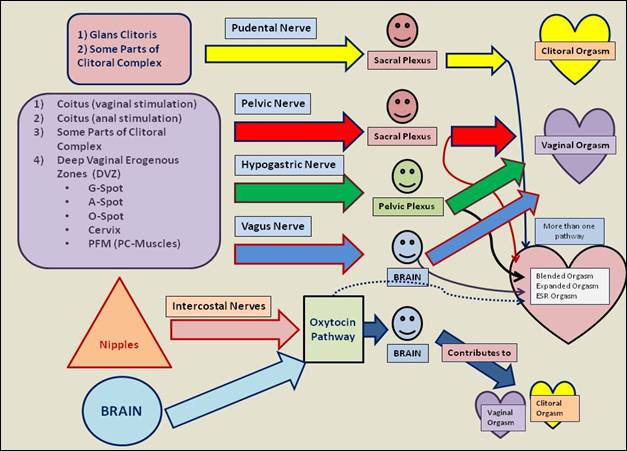
Figure 10. Four Nerve Six Pathway Theory of Female Orgasm. At least six pathway-orgasmic reflex arch systems work during the development of female orgasms. Pudental, Pelvic, Hypogastric, intercostal and Vagus nerves constitute the main nerve network system. Also there are at least two Oxytocin pathway systems, whereas Oxytocin works as a neurotransmitter and as a hormone, separately. During expanded orgasms and ESR orgasms, more than one ‘orgasm reflex arch pathway’ is activated and trigger an expanded orgasm, while many others contribute to the formation of an EO or ESR orgasms.
If there are six orgasmic pathways to trigger an orgasm, then female orgasm can be triggered in 63 ways; among them, 57 of them would be blended or ESR orgasms. If the above 14 loci take part in the development of an orgasm, then there are (214 -1 = 16283) combinations or possibilities of factors, that supply complementary orgasmic input into the brain. This theory may explain why female orgasms are so diverse, and why it is very difficult to understand and explain the patterns of female orgasms. According to this theory, during the development of a particular type of orgasm, the other pathways or loci may supply additional sensory input and pleasure information into the brain until an orgasm reflex is triggered. For the development of clitoral orgasms, for instance, the triggering locus is glans clitoris and the main reflex arch is pudental nerve-sacral plexus orgasm reflex arch, whereas the orgasm trigger command is given by the neocortex and limbic system. During the development of a clitoral orgasm, however, other loci and pathway systems may also carry supplementary pleasure input into the pleasure centers of the brain and the neocortex. In expanded orgasms or ESR orgasms, more pleasure input is carried through many loci and many pathways systems, such that at least two or more, orgasm reflex pathways are activated at the same time, while many other loci and pathways carry lots of supplementary information into the brain, such that orgasmic response is stronger, more intense, prolonged and more pleasurable, lasting for from a couple of minutes to tens of minutes, or even hours (Rhodes, 1991; Schwartz, 1999; Bodansky, 2000; Taylor, 2000, 2002; Zdrok, 2004; Sayin, 2010, 2012a, 2013). This is just like the “opening of the doors of perception”, namely “opening of the doors of the orgasmic perception and orgasmic consciousness”. In ESR orgasms, the intensity, duration and pleasure increases by time and by the course of orgasmic train, as described by many women; for instance, the fifteenth orgasm is much more intense and prolonged than the fifth orgasm, once the orgasmic train commences and continues, as depicted in the plot in Figure 1-B. Many women have described transcendental, mystical, ASC experiences during an EO or ESR orgasm, which is a proof that ESR orgasms are novel doors opening to another “orgasmic consciousness”, which lasts for a very long time, compared to classical single orgasms recorded in the literature (Taylor, 2000, 2002; Sayin, 1993, 2010, 2012a, 2013).
Discussion
Orgasmic Consciousness
Female orgasm has been defined as a form of ASC by many researchers (Fisher, 1973; Davidson, 1980; Taylor, 2000, 2002; Mah, 2002, 2005; King, 2010; Sukel, 2011; Sayin, 2010, 2011c, 2012a-b, 2013). King, Mah & Binik categorized subjective feelings of female orgasms in 10 dimensions as building sensations, flooding sensations, flushing sensations, shooting sensations, throbbing sensations, general spasms, pleasurable satisfaction, relaxation, emotional intimacy, and ecstasy (King, 2010). Taylor classified her cases into four dimensions as physical, mental, emotional and spiritual. Taylor’s cases described a deep experience of ASC such as, more pleasure; deep relaxation; heightened sensations; increased energy; temporary pain relief; energy expanding out of body; deep relaxing abdominal breathing; increased clarity and creativity; acceptance of the self and others; extra sensory perception; ecstasy; mystical experience; divine feelings; increased awareness of the body; mind connection and integration; psycho-spiritual birth and death experience; loss of illusion of spatial separation; loss of spatial dimensions, loss of sense of time; personal boundaries dissolving and merging with the divine; cosmic emptiness and void; sharing with the partner; compassion; sense of fulfillment etc. (Taylor, 2000). In our study, which is still continuing, we have distinguished 85 psychological effects during intense and prolonged orgasms, as we have reported before (Sayin, 2011c, 2012a-d, 2013; See Table-1). In our study we also separated single orgasms from, prolonged-multiple-intense ESR orgasms; evaluating them as two separate entities. Although in classical single orgasms, there are sometimes sharp psychological changes and ASCs; we have come to the conclusion that most of piercing psychological shifts of the mood and most of the ASCs occur during intense and prolonged ESR orgasms. The main mechanism of such alterations of mood can only be explained by the “ecstatic activation” of various centers of the brain and release of many neurotransmitters in various parts of the brain during intense and prolonged orgasms; such as endogenous opiates, dopamine, serotonin, oxytocin, norepinephrine, glutamate, and prolactin. It is, already, reported that during a single orgasm developing by masturbation or by intercourse, dopamine (Stahl, 2001; Kruger, 2006; Passie, 2005; Brown, 2007), prolactin (Kruger, 2002, 2005; Passie, 2005;), oxytocin (Stahl, 2001; Argiolas, 2003; Passie, 2005; Krüger, 2006), melanocortin (Brown, 2007), serotonin (Stahl, 2001; Brown, 2007) norepinephrine (Stahl 2001) and endogenous opioid peptides (Argiolas, 2003) are released and involved in the mechanisms of altered “orgasmic consciousness”. Acute dopamine, the pleasure neurotransmitter, release is a ‘satisfaction and bliss’ factor during the female orgasms (Stahl, 2001; Komisaruk, 2006; Brown, 2007). For such an alteration, involvement of more than one orgasmic reflex pathway can be one of the mechanisms, whereas the physiological changes during a female orgasm is doubled or tripled, by the stimulation and activation of many reflex centers. “Four nerve and six pathway theory of female orgasm” seems to be a better model to explain the sharp changes of the consciousness, while oxytocinergic pathways play a major role. We have also investigated the acute behavioral effects of intranasal oxytocin spray (10 IU) in a group of women, compared with the placebo: our results were confirming this hypothesis, because intranasal oxytocin (1o IU), alone, induced ASC-like symptoms in 9 women (30.7 %); subjective feeling of analgesia in 9 women (30.7 %); happiness, calmness, serenity, euphoria in 15 women (57.6 %) and sexual arousal in 10 women (38.4 %) out of 26, within 10 minutes after administration. There were no such effects after the placebo, which was administered to the same person either before or after oxytocin administration in a double blind fashion (Sayin, 2012g ).
|
Table 1. Psychological Effects and ASCs Induced by Enhanced, Expanded and ESR Orgasms |
||
|
1) Pulsating feeling |
30) Feeling of fulfilling, achieving something |
59) Feeling wild, becoming wild |
|
2) Throbbing feeling |
31) Losing oneself |
60) Feeling animal, animalism |
|
3) Tickling |
32) Exploding |
61) Seeing different colors |
|
4) Warm, warmth feeling |
33) Volcano |
62) Seeing flaring of lights |
|
5) Hot, very hot feeling |
34) Ecstatic |
63) White or colored flashes |
|
6) Physical warmth |
35) Unify, Unified feeling |
64) Seeing different geometrical objects |
|
7) Spiritual warmth |
36) Unifying with the partner |
65) Feeling the body and mind extraordinary |
|
8) Exciting |
37) E extreme feelings of love and bursts of love to the partner |
66) Travelling to different lands, e.g. evergreens, forest, waterfalls, gardens etc |
|
9) Pleasurable |
38) Attachment to the partner |
67) Voyage to unknown places |
|
10) Quivering |
39) Cessation of time, time stops |
68) Finding one’s self in different lands, e.g. evergreens, forest, waterfalls, gardens etc. |
|
11) Shuddering |
40) Distortion in space-time continuum |
69) Dissolving into the partner |
|
12) Earth quake feeling |
41) Flowing feeling |
70) Unifying with environment and universe |
|
13) Flushing |
42) Flooding feeling |
71) De ja vu |
|
14) Euphoric |
43) Absorbed feeling |
72) Unreal feeling |
|
15) Uncontrolled feeling |
44) Immersing feeling |
73) Surreal feeling |
|
16) Elevation of mood |
45) Swelling feeling |
74) Opening into a surreal universe |
|
17) Elated |
46) Dissolve feeling |
75) Seeing Cartoon characters, short cartoon movie |
|
18) Rapturous |
47) Crying |
76) Blissful feeling |
|
19) Losing oneself |
48) Giggling, laughter |
77) Mystical experience |
|
20) Intense LOVE |
49) Rising, going up |
78) Cessation of breathing, not to be able to breath for a long time |
|
21) Extreme excitement |
50) Out of body experience |
79) Resolving of pain (Analgesic Effect) |
|
22) Close to herself, environment) |
51) Fly, flying |
80) Subsiding and decreasing of depression (Anti-Depressant Effect) |
|
23) Close to the partner |
52) Astral voyage |
81) Release from anxiety, decreasing of existing anxiety (Anxiolytic Effect) |
|
24) Peaceful |
53) Death feeling |
82) Increase of enthusiasm and creativeness |
|
25) Spurting feeling |
54) Near death experience |
83) Feeling of relaxing of muscles, decreasing tension in muscles(Myo-relaxant Effect) |
|
26)Relaxing |
55) Spreading feeling |
84) Soothing and sedating effect; release from tensions and stress (Sedating Effect) |
|
27) Filled |
56) Depersonalization |
85) Happiness during and after orgasm , Feeling extremely content (Anti-depressant effect) |
|
28) Peacefully relaxing |
57) Losing the soul feeling |
|
|
29) Soothing |
58) Soul outside |
|
A sample description of an ESR orgasm we have recorded in our surveys may clarify and visualize the “orgasmic consciousness” of a woman (Sayin, 2010):
J. K. is a medical doctor. She is 36 years old. She had her first sexual intercourse at the age of 16, she had her first vaginal orgasm at the age of 24, when also she discovered her G-Spot. She started to have expanded orgasms and status orgasmus at the age of 28. She had nearly 40-50 partners since she was 16. Her score from ESR-Scale was 132/150 (in 2011). She says that she has been hypersexual since she was 26. She adds that she has been practicing Kegel Exercises since she was 26. She has not been diagnosed for any psychiatric disorder:
During my orgasms I depart from everything around, it is a total depersonalization. I just feel myself, I even forget myself. Only my voice and screams stay. In status orgasmus, which are my best to be satisfied, the pleasure increases gradually, I am totally isolated from my environment. Only I hear the animal voice coming from my throat, my short moans turn out to be incredible screams. I feel it on my stomach, first some tingling, then the contractions follow each other. It is a total altered state of consciousness. My vision darkens; I see flashes of colors or light. During minor orgasms I feel funny contractions, like a game. The minor orgasms or contractions starting from my vagina and pubis circulate through my stomach, where I can feel the real center of the orgasmic volcano. Once status orgasmus starts, it is like a hurricane taking me away from my body and I fly, these minor orgasms each lasting for nearly 10 to 20 seconds, build up into a continuous tetanic fit, while I sometimes can’t hear my screams, I am lost in the first few minutes. These contractions continue for 10-20 minutes especially when my partner is doing oral sex (cunnilingus) on me. He continuously stimulates my clitoris by his tongue so talented that one orgasm finishes, other begins. During a status I feel that I am traveling the world, as if I have an astral body, I go to unknown gardens, waterfalls, meadows. During intercourse orgasms I feel an unbelievable unification and merging, and dissolving in each other. I also had status orgasmus during intercourses. If my partner continues intercourse for 1-3 hours, it is easy to attain prolonged orgasms. My brain melts, I realize that I am an animal; I hear my animal voices coming from my throat which make me more excited. Vaginal orgasms are sometimes better than clitoral. While we also apply a message vibrator during the intercourse, I easily go into the status orgasmus which lasts for ten minutes to half an hour, while I experience nearly 50-60 minor orgasms. During orgasms I laugh, cry, moan, make very loud noises (always I am afraid that neighbors may hear me!) my body arches, I am in full extension, it is sometimes not certain whether I having pain or pleasure. Fantasies whispered to my ear make me crazy during these orgasms. Even a word may start another minor orgasm. It could be anything, wild or soft; I want to become an animal, return to my archetype body whatever it had been. When I contract, I feel like an animal, as if it comes from my collective sub consciousness. I feel the penis like a hot, burning sword that brands me. Makes my pelvis hotter and hotter, it steams out, and then comes a huge contraction, following another. Status orgasmus is very satisfactory for me, compared to other orgasms, like the ones due to the clitoral or vaginal stimulation alone. I feel so dizzy and my brain is so high and turning around that I believe it would be very hard for me walk on a straight line, I would fall. I love to lose myself in my own brain chemistry. I would not be satisfied if I did not experience status, because clitoral or vaginal minor orgasms are so low for me. They don’t make me as high as the status orgasmus does. I don’t have any refractory period for attaining vaginal or clitoral orgasms. One may come after another without building into a status orgasmus. But for the status, there is always a refractory period of 15-20 minutes (truncated)…
Expanded Orgasms and ESR
Taylor has reported that the expanded orgasm (EO) or ESR orgasm duration was 0.2 to 60 minutes in 22 female subjects (a total of 44 subjects or 22 couples), while the average EO duration was 7.2 hours (Taylor, 2000). Although Taylor’s data seems to be difficult to believe and we have never come across such extreme cases; in our study, the women who experienced ESR orgasms proclaimed that during a status orgasmus or prolonged ESR orgasm, which lasted from a couple of minutes to 10-15 minutes or more, they had had 20 to 30 minor orgasms in a train of multiple orgasms during the “orgasmic consciousness” (Sayin, 2012a, 2013). These figures are beyond the published limits and the normal recorded physiology of the female orgasm; however it is a fact to be investigated and explained by neuroscience. According to ‘Cosmo Report’ among 10 000 American women, 14.8 % of women could attain only one orgasm, 65.9 % could have 2 to 5 orgasms, 13.4 % could reach to 6 to 10 orgasms, while only 5.9 % could attain 11 or more orgasms during one love making session (Wolfe, 1982). Our surveys point out that 2.1 % (Kadınca Report, 1993; N=1534), 4.7 % (Hülya Report, 2003; N=706) and 4.3 % (Istanbul Report, 2013, continuing; present N= 470) of Turkish women can attain more than 11 orgasms during a love making session (Sayin, 2010, 2011d, 2013). Thus, in different cultures we have substantial data which confirms the existence of a group of nearly 4-5 % of women who can attain more than 11 (up to 20 or more) orgasms in a couple of hours. Depending on the data from many other worldwide surveys made us to work on a mathematical model to make an assumption that a proportion of 10 to 15 % of women can attain ESR orgasms by training and education, while an average of 1-3 % are, most probably, experiencing the extreme “orgasmic consciousness” mentioned above, at present (Sayin, 2012a-b, 2013).
ESR and Deep Vaginal Erogenous Zones
Our study on ESR points out that, for experiencing extreme orgasmic consciousness, a woman; 1-Should attain and experience multiple clitoral, vaginal and blended orgasms separately. 2- Should use her PFM (PC-Muscles) during sexual response and should possess developed, powerful PFM. 3-Should have a developed masturbation pattern. 4- Should have a developed “sexual-brain”. 5- Should be aware of her G-Spot and DVZs, experiencing G-Spot or DVZ orgasms. 6-Should be using novelties, variations and sex toys (e.g. various types of vibrators, vibes) to discover herself and to attain more pleasure in her sexual life style (Sayin, 2012a-b, 2013). DVZ was first defined by the famous British zoologist Desmond Morris (Morris, 2004); however, the pleasurable sensitivity of anterior and posterior walls of vagina have been reported for a long time by many researchers, since Sigmund Freud (Reich, 1973; Singer, 1973; Fisher, 1972, 1973; Kaplan, 1981; Ladas, 1982; Britten, 1983; Whipple, 1988; Bancroft, 1989; Escapa, 1989; Komisaruk, 2003, 2004, 2005, 2006; Zdrok, 2004; Carellas, 2007; Sayin, 1993, 2010, 2011a-b-c, 2012a-b-c-e). Although the nervous innervations of pelvic nerve and hypogastric nerve in the walls of vagina are not well established anatomically and histologically, Whipple et al, reported that self-stimulation of anterior and posterior walls of vagina induced pleasure and analgesia, as much as the stimulation of the clitoris (Whipple, 1988). If there is pleasure and analgesia, then there should be some zones innervated by peripheric nerves that carry messages of pain, pressure, vibration etc. The phenomenon, Whipple et al. had observed, could be a result of the analgesic effects of acute oxytocin and endorphin release, which is secreted by the stimulation of clitoris, vaginal walls, cervix, uterus or DVZ, and during a female orgasm, as we also have reported (Sayin, 2012a-g). Those zones at the anterior and posterior walls of vagina can be G-Spot, A-Spot, O-Spot, and probably cervix, while most of the women cannot pinpoint the sensation originating from deep vaginal structures in correct coordinates. A proof for this hypothesis came from a recent survey among 5000 British women in England (2011), as mentioned above (http://www.orgasmsurvey.co.uk/pressrelease.htm), 1260 women out of 5000 (25.2 %) described pleasurable zones at the vaginal walls as “G-Spot”, while they described the coordinates of G-Spot incorrectly, since the questionnaire did not have the choices of other DVZ areas.
Awareness of DVZs (G-Spot, inner clitoris, A-Spot, O-Spot, Cervix, PFM) is very important for developing ESR, and many ESR women are aware of those pleasurable areas, as our surveys on ESR, has found out (See figure-6; Sayin, 2012a-b-c). Our other research also revealed that some areas in deep vagina were sensitive to high frequency vibration (80 Hz to 160 Hz), which is not experienced by traditional vibrators, having a vibration frequency of nearly 40-60 Hz. and also, when stimulated by galvanic current using a TENS unit, these DVZ areas induced sexual pleasure and occasionally orgasm in some women (unpublished data). We have recently described a method to induce prolonged blended orgasms in women who have achieved the state of “orgasmic consciousness” and ESR, which can be used in sex therapy (Sayin, 2012a, 2013).
A Special Method for Sex Therapy to Induce Expanded ESR Orgasms in Women. Four Spot Method: In the women who have developed ESR, an effective method is described to induce prolonged orgasms: Stimulation of G-spot (coitus, manual, electrical or vibe), Deep Vaginal Erogenous Zones (DVZ) (coitus, vibe , electrical, or manual), glans clitoris (cunnilingus, manual, vibe, or electrical), clitoral complex (coitus, vibe, electrical, or manual), anus (coitus, vibe, or manual) , nipples (mostly manual, labial or vibe) and the brain (fantasies, images, thoughts, sexual pleasure objects, learned sexual behavior patterns) at the same time, may start to induce blended orgasms in a minority of women after certain numbers of trials, by means of triggering more than one orgasm reflex pathways. The vibration frequency of effective vibes (vibrator dildos) differs from spot to spot (60-200 Hz); also, vibe frequency may be variable in different women. For coitus, a male partner should be maintaining intercourse for more than 30 minutes. For oral sex, a continuous stimulation more than 20-30 minutes should be maintained In Four Spot Method, male partner uses his left hand’s second and third fingers to stimulate the G-Spot upward, fourth finger of the left hand is used to stimulate anus. The head is in between the legs of the woman to perform cunnilingus, which should be continued for at least 30 to 40 minutes, with up and down (sometimes left and right) continuous movements of the tongue (1-3 Hz). The right hand should be stimulating the left nipple of the women (Sayin, 2012a). Thus anus, G-Spot, glans clitoris, nipples are stimulated at the same time until she reaches a series of orgasms, which may last for more than 2-15 minutes. In between these stimulations, rotating probe and vibrating vibes can be used to stimulate the DVZ.
Why Should We Do Research on ESR Phenomenon?
Only 130-140 years ago, a woman’s questioning and mentioning about female orgasm was a taboo in many cultures. In England, during the Victorian Era, women were prohibited to masturbate and to get pleasure from sex, while doctors made them wear weird chastity belts at nights to prevent them from masturbation and sexual pleasure, claiming that masturbation, pleasure and orgasm were harmful for the good women’s psychology (Escapa, 1989; Sayin, 2010, 2012a). After the publications of Havelock Ellis, Kraft Ebbing, Sigmund Freud, Van de Valde, Wilhelm Reich, Erich Fromm, Alfred Kinsey and Masters & Johnson, female sexual pleasure, masturbation, and female orgasm were started to be accepted as normal and healthy physiological entities. However, ancient cultures had investigated the limits and possibilities of female pleasure and orgasm in the Far East (Chang 1977, 1983; Wu, 1996; Schwartz, 1999; Chia 2002, 2005; Mamford, 2005; Michaels 2008; Sayin, 2012a); Tantrists and some Taoists had developed some unique and specific techniques to enhance female pleasure and orgasm centuries ago. Although defined in medical literature recently, those cultures were aware of the ESR phenomenon; which means that we are re-discovering the ESR in West in this century! Even recently, the debate about the existence of G-Spot has lasted for 30-40 years, while today there are still some physicians and researchers who do not believe that G-Spot exists in some women. In this very conservative world, it is very difficult to establish some novel facts, even though they are reported by many researchers and scientists; however, the only way to be aware of those facts is to investigate and to continue doing research!
Some authors state that the re-discovery and research of female orgasm is a revolutionary process in the new enlightenment age and is a litmus paper for being civilized (Tannahill, 1992; Muchembled, 2008). Investigating the extents and limits of female climax, sexual peak experiences and “orgasmic consciousness” is not for only the benefit of the women, but particularly for the men, also! Discovery of the mechanisms of the normal sexual physiology, as well as the extents and limits of it, can be utilized for a better sexual life and happiness of women and men in the 21st Century; while, many sexual disorders can be treated in a better context. ESR is a learned phenomenon and many women and men can learn how to attain it by training and education.
Four Nerve and Six Pathway Theory of Female Orgasm: A Unified Theory?
Glans clitoris is an orgasm triggering locus for many women (Masters & Johnson, 1966; Kaplan, 1981). However, it is not easy to talk the same way about the other erogenous zones for the majority of women. Fifty to sixty percent of women in many cultures are not aware of their G-Spots, and nearly two third of the female population cannot experience vaginal orgasms (Hite, 1976; Wolfe, 1982; Sayin, 2010, 2011b, 2012a); the awareness of other recently proposed DVZs is much less. DVZs, in average women may contribute to the building up of an orgasm by means of supplying additional and supplementary erogenous information input into the brain, however, the sensory input in ESR women from the DVZs, is much more and enhanced, even to trigger an orgasm from each DVZ, e.g. triggering an orgasm from the stimulation of G-Spot, A-Spot, Cervix, PFM etc. alone, while they may only serve as a complimentary erogenous zone in the development of an orgasm in many women.
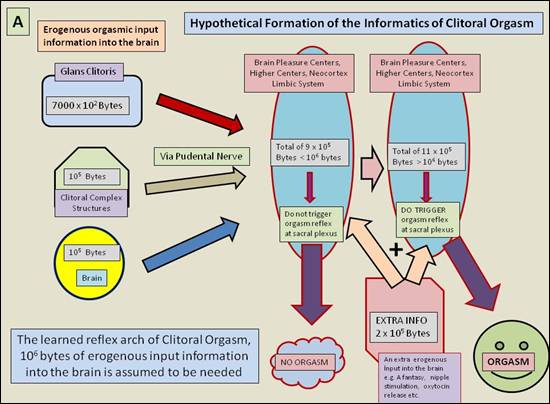
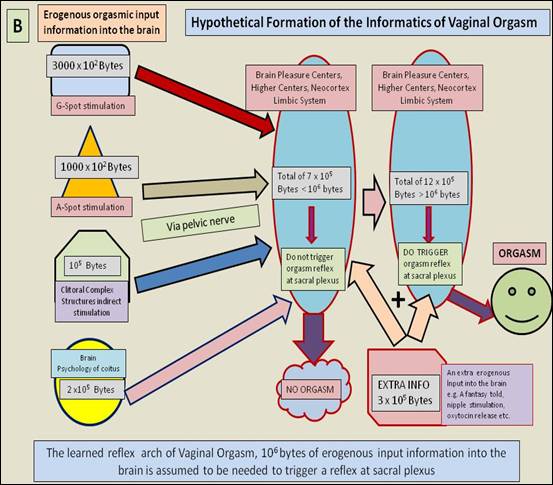
As a mathematical model, let’s assume that the amount of erogenous information input to trigger an orgasm in the brain is 106 bytes (Figure 11). In either clitoral, vaginal or blended orgasms, the erogenous input information into the brain is shared by many components, e.g. brain’s perception, input from glans clitoris, love making, other erogenous zones, psychological sexual molds, fantasies, sexual pleasure objects etc. If the erogenous input information overflows a certain amount of input, e.g. exceeds 106 bytes of information, that is needed to trigger an orgasmic reflex arch at one of the orgasm centers of the spinal cord or the brain, then the brain gives the order to trigger an orgasm. In this model the sensory and psychological input serve as positive information in favor of orgasm, while psychological inhibitions, learned psychological taboos, obstacles and clogs, may play an anti-orgasmic role against orgasm, attenuating the effects of the sensory erogenous input information in the dynamics of inner psychology and subconsciousness; namely, the brain can learn orgasming, as well as un-orgasming, or psychologically clogging pleasure or orgasms, which may lead to sexual function disorders, such as anorgasmia, hyposexuality and vaginismus.
A schematic model is described in the drawings of Figure-11, to symbolize this complementary sharing. All the process is a learned reflexive behavior. In clitoral orgasms, glans clitoris plays the major role, while the stimulation of the clitoris may or may not be sufficient to trigger an orgasm which is learned during the growth of the women by trial and error, since glans clitoris is outside the body and reachable. Sometimes stimulation of glans clitoris is not sufficient and other erogenous sensory input information may be needed, which can be supplied by other components of four nerve and six pathway system (e.g. additional oxytocin release, by means of sucking or stimulating the nipples) or fantasies and particular erotic thoughts.
In vaginal orgasms, there may be more components to trigger an orgasm, such as, DVZ areas or other psychological input from the brain itself. In average women (NESR-women), such extra informational input can be supplied from many other pathways cited in this article, particularly orgasmic four nerve-six pathway system. In ESR women, all the components in four nerve-six pathway system is enhanced and carry more sensory sexual information input, and probably the number of sexual components are increased too, which is observed in our surveys such as that the fantasy, masturbation, sexual image, libido patterns are enhanced and expanded in ESR women. Thus, ESR women have learned more orgasm inducing pathways to be sufficient to trigger an orgasm alone (e.g. to become orgasmic through the activation of each pathway alone). Hence, ESR orgasms are enhanced and prolonged, since they carry more sexual erogenous information input from more than one orgasm inducing pathway into “a more sexually excitable brain and psychological system”. However, in NESR women only one systematic orgasmic pathway works, and that is, most of the time, the clitoral orgasm pathway through pudental nerve, the other orgasm inducing pathways in NESR women only function as complementary, and supply additional sensual information to facilitate the building of an orgasm through one pathway, e.g. clitoral-pudental-sacral plexus orgasm pathway. The brain and the body of ESR women function in a more sophisticated and evolved fashion, while many novel components to the four nerve-six pathway system may be added. In ESR women, the learned orgasmic reflex pathways are enhanced and increased; e.g. ESR women can attain orgasms by means of the stimulation of glans clitoris, coitus, sole stimulation of DVZs or by contracting PFM (PC-Muscles) etc. So four nerve-six pathway theory is a more likely to explain ESR phenomenon. In ESR women the following pathways may induce orgasms separately, while they may only play as a contributing and complementary role in NESR to build up an orgasm. Dopaminergic, oxytocinergic, serotoninergic, glutamatergic, endogenous opioid systems also play an auxiliary role in the development of orgasms through these pathways:
1-Glans clitoris-Pudental nerve-sacral plexus
2-Coitus-DVZs-Pelvic nerve-sacral plexus
3-Coitus-DVZs-cervix-Hypogastric nerve-pelvic plexus
4-Coitus-DVZs-uterus-cervix-Vagus nerve-brain
5-Nipples-intercostal nerves (particularly T-4)-pituitary-oxytocin pathway (oxytocin as a hormone)
6-Brain-fantasies-sexual images-sexual psychology-frontal, somatosensory, prefrontal cortices-limbic system- hypothalamus-pituitary-oxytocin pathway (oxytocin as a neurotransmitter).
“Four nerve and six pathway theory of female orgasm” seems to explain some of the characteristics of ESR. ESR is novel phenomenon to be investigated by neuroscience in 21st Century, since many women can have a better quality of sex life, pleasure and orgasms, after certain training, if the basic mechanisms of ESR are discovered. More detailed research should be carried for the investigation of ESR, EO and female orgasm, as well as the neurophysiology and neuroanatomy of female sexual response to grant a more healthy and pleasurable life to both women and men.
Figure 11. Hypothetical Informatics Model for the Formation of Clitoral and Vaginal Orgasms in Four Nerve and Six Pathway Theory. The psychological sexual sensory input that leads up to the development of an orgasm reflex is shared by many components, while psychological inhibitions, taboos play an inhibiting role of the orgasmic input, as anti-orgasmic. All the process is a learned reflexive behavior. A schematic model is described in the drawings, to symbolize this complementary sharing.
A) In clitoral orgasms, glans clitoris plays the major role, while the stimulation of clitoris may or may not be sufficient to trigger an orgasm. Other erogenous sensory input information may be needed, which can be supplied by other components of four nerve and six pathway system (e.g. additional oxytocin release).
B) In vaginal orgasms, there may be more components to trigger an orgasm, such as, DVZ areas or other psychological input from the brain itself. In average women (NESR-women), such extra information input can be supplied from many other pathways cited in this article, particularly orgasmic four nerve-six pathway system. In ESR women, all the components in four nerve-six pathway system are enhanced and carry more sensory sexual information input, and probably the number of sexual components are increased too; and ESR women have learned more orgasm inducing pathways to be sufficient to trigger an orgasm alone, e.g. to become orgasmic through the activation of solely each pathway. Hence, ESR orgasms are enhanced and prolonged, since they carry more sexual erogenous input information from more than one orgasm inducing pathway, while in NESR women only one systematic orgasmic pathway works, and that is the clitoral orgasm pathway through pudental nerve, the other orgasm inducing pathways in NESR women only function as complementary, and supply additional information to facilitate the building of an orgasm through one pathway, e.g. clitoral-pudental-sacral plexus orgasm pathway. Note that the constituents given by geometrical shapes at the left side of the two figures are only for schematic purposes, there are of course more components, not only the ones that are shown.
References
Addiego F, Belzer EG, Comolli J, Moger W, Perry JD, Whipple B. Female ejaculation: a case study. J Sex Res 1981; 17 (1): 13–21.
Argiolas A, Melis MR. The neurophysiology of the sexual cycle. Endocrinol Invest 2003; 26 (3 Suppl): 20-2.
Armagan N, Sayin HÜ, Kocatürk A. Can Sexual Response be Enhanced and Expanded in the Human Female: Preliminary Findings and a Proposed Psychometric Scale for Expanded Sexual Response (ESR). 38th Annual Meeting of IASR (International Academy of Sex Research), Lisbon-Portual, July 8-11, 2012; Abtract Book, 38: 9.
Alzate H. Vaginal eroticism: a replication study. Arch Sex Behav 1985; 14: 529 –537.
Bancroft J. Human sexuality and its problems. New York: Churchill Livingstone, 1989.
Belzer EG. Orgasmic expulsions of women: a review and heuristic inquiry. J Sex Res 1981; 17 (1): 1–13.
Bodansky S, Bodansky V. Extended Massive Orgasm, California: Hunter House Pub, 2000.
Britten B. The Love Muscle: Every Woman’s Guide to Intensifying Sexual Pleasure, N.Y.: Signet Books, 1983.
Brown AD, Blagg J, Reynolds DS. Designing drugs for the treatment of female sexual dysfunction. Drug Discov Today 2007; 12 (17-18): 757-66.
Brody S, Krüger TH. The post-orgasmic prolactin increase following intercourse is greater than following masturbation and suggests greater satiety. Biol Psychol 2006; 71(3):312-315.
Campbell B, & Petersen WE. Milk ‘‘let-down’’ and the orgasm in the human female. Human Biology 1953; 25: 165–168.
Carellas B. Urban Tantra. New York: Celestial Arts, 2007.
Chang J. The Tao of Love and Sex : The Ancient Chinese Way to Ecstasy. New York: Dutton, 1977.
Chang J. The Tao of the Loving Couple: True Liberation Through the Tao. New York: Dutton, 1983.
Chia M, Chia M, Abrams M, Abrams RC. The Multi-Orgasmic Couple: Sexual Secrets Every Couple Should Know. New York: Harper One, 2002.
Chia M. Healing Love through the Tao: Cultivating Female Sexual Energy. New York: Destiny Books, 2005.
Davidson JM, Davidson R J. The psychobiology of consciousness. New York: Plenum Press, 1980.
Davidson J K Sr, Darling C A, Conway-Welch C. The role of the Grafenberg spot and female ejaculation in the female orgasmic response: an empirical analysis. J Sex & Marital Ther 1989; 15:102– 120.
Deadone Nicole. Slow Sex: The Art and Craft of Female Orgasm, Boston: Grand Central-Life Style, 2011.
Escapa Roy, Bizzare Sex, London: Grafton Books, 1989.
Fisher S. Female Orgasm, New York: Basic Books, 1972.
Fisher S. Understanding the Female Orgasm, London: Penguin Books, 1973-1977.
Glenn J & Kaplan EH. Types of orgasm in women: a critical review and redefinition. J Am Psychoanaly Ass 1968; 16: 549 –564.
Hite S. The Hite Report: A National Study of Female Sexuality. New York: Dell Publishing, 1976.
Hooper R. New Scientist, February 20th, 2008; 2644:6-7.
Kaplan HS. The New Sex Therapy, New York: Penguin Books, 1981.
King R, Belsky J, Mah K, Binik YM. Are there different types of female orgasms? Arch Sex Behav 2010; 40(5):865-75.
Kline-Graber G, Graber B. A guide to sexual satisfaction: woman’s orgasm. New York: Fawcett Popular Library. 1975.
Kocatürk A, Sayin HÜ, Baş GY, Kocatürk C. Comparison of the Sexual Behavior of 939 Female Students in İstanbul Universities (2012) to the Survey Results of Kadınca Report (1993): Decline in Sexual Knowledge and Education in Turkish Universities? 38th Annual Meeting of IASR (International Academy of Sex Research), Lisbon-Portual, July 8-11, 2012; Abtract Book, 38: 82.
Komisaruk BR, Sansone G. Neural pathways mediating vaginal function: The vagus nerves and spinal cord oxytocin. Scandinavian J Psych 2003; 44:241-250.
Komisaruk BR, Whipple B, Crawford A, Grimes S, Liu WC, Kalnin A, Mosier K. Brain activation during vaginocervical self stimulation and orgasm in women with complete spinal cord injury: fMRI evidence of mediation by vagus nerves. Brain Res 2004; 1024:77-88.
Komisaruk BR, Whipple B. Functional MRI of the brain during orgasm in women. Annu Rev Sex Res, 16: 62-86, 2005.
Komisaruk BR, Beyer-Flores C, Whipple B. The Science of Orgasm, Baltimore: John Hopkins University Press, 2006.
Krüger TH, Haake P, Hartmann U, Schedlowski M, Exton MS. Orgasm-induced prolactin secretion: feedback control of sexual drive? Neurosci Biobehav Rev 2002; 26(1):31-44.
Krüger TH, Hartmann U, Schedlowski M. Prolactinergic and dopaminergic mechanisms underlying sexual arousal and orgasm in humans. World J Urol 2005;23(2):130-8.
Krüger TH, Schiffer B, Eikermann M, Haake P, Gizewski E, Schedlowski M. Serial neurochemical measurement of cerebrospinal fluid during the human sexual response cycle. Eur J Neurosci 2006; 24(12):3445-52.
Ladas AK, Beverly W, Perry JD. The G-Spot and other Discoveries About Human Sexuality, New York: Henry Holtand Company 2005, (first publication 1982).
Mah K, Binik YM. The nature of orgasm: A critical review of major trends. Clin Psych Rev 2001; 6:823-56.
Mah K, Binik YM. Do all orgasms feel alike? Evaluating a two-dimensional model of the orgasm experience across gender and sexual context. J Sex Res 2002; 39:104113.
Mah K, Binik YM. Are orgasms in the mind or the body? Psychosocial versus physiological correlates of orgasmic pleasure and satisfaction. J Sex & Marital Ther 2005; 31:187-2005.
Mamfurd J. Ecstasy through Tantra. Minnesota: Llewellyn Pub, 3rd ed., 2005
Masters W, Johnson V. Human Sexual Response, Boston: Little Brown Company, 1966.
Masters W, Johnson V. Human Sexual Inadequacy, Boston: Little Brown and Company, 1970.
Masters W, Johnson V, Kolodny RC. Human Sexuality (textbook), New York: Harper Collins, 1995.
Morris D. The Naked Woman: A Study of the Female Body. London: St. Martin's Griffin, 2004.
Muchembled R, Ferbach D (tr). Orgasm and the West: A History of Pleasure from the 16th Century to the Present, New York; Polity, 2008.
Passie T, Hartmann U, Schneider U, Emrich HM, Krüger TH. Ecstasy (MDMA) mimics the post-orgasmic state: impairment of sexual drive and function during acute MDMA-effects may be due to increased prolactin secretion. Med Hypotheses 2005; 64(5):899-903.
Perry JD, Whipple B. Pelvic muscle strength of female ejaculators: evidence in support of a new theory of orgasm. J Sex Res 1981; 17 (1): 22–39.
Reich W. The function of the orgasm: sex – economic problems of biological energy. New York: Farrar, Straus and Giroux (V.R. Carfagno, Translation; original work published 1942), 1973.
Reubens JR. The physiology of normal sexual response in females. J Psychoactive Drugs 1982; 14: 45 –46.
Rhodes R, Brauer A, Brauer DJ. ESO Ecstasy Program: Better, Safer Sexual Intimacy, New York: Grand Central Publishing, 1991.
Sayin HÜ. Other Dimensions of Sexuality (Cinselliğin Farklı Boyutları), İstanbul: YOL Publications, 1993.
Sayin HÜ. Deep Sex: Different Dimensions and Openings of Sexuality (Derin Seks: Cinsellikte Farklı Boyutlar, Yeni Açılımlar), İstanbul: Klan Publications, 2010.
Sayin HÜ, Ramstadius M, Kocatürk A. Expanded Desire: The Main Parameters and New Definitions of Enhanced and Expanded Sexual Response (ESR). The 33rd NACS Conference 2011, Oslo, Norway. Abstract Book, 33:21, 2011. (a)
Sayin HÜ, Ramstadius M, Kocatürk A. Pelvic Floor Muscle Strength is Correlated with Attaining Vaginal Orgasms in Human Female as Measured by Kegel Perineometer. The 33rd NACS Conference 2011, Oslo, Norway. Abstract Book, Abstract Book 2011; 33: 22, 2011. (b)
Sayin HÜ. Altered states of consciousness occurring during expanded sexual response in the human female: preliminary definitions. Neuroquantology; 9(4): 882-891, 2011. (c)
Sayin HÜ, Can G, Ramstadius M, Kocatürk A, Kahya I. Orgasmic Behavior Patterns in 2240 Educated Turkish Women Which Improves with Education. The 33rd NACS Conference 2011, Oslo, Norway. Abstract Book, Abstract Book 2011; 33: 22, 2011. (d)
Sayin HÜ. Expanded Sexual Response (ESR): Ultra Orgasm in Women (Artırılmış Cinsel Doyum: ESR). İstanbul: Tantra Akademi Publications, 2012. (a)
Sayin HÜ, Kocatürk A. Expanded Sexual Response in the Human Female: The Mechanisms of Expanded Orgasms in Women (Review). Proceedings of NACS-2012-Helsinki Conference, Proceedings Book 2012; pp:147-163 (available at: http://www.expandedorgasms.net/pdf-sayin-etal/sayin-nacs-proceeding-paper-02.pdf ) (b)
Sayin HÜ, Kocatürk A, Armagan N. What Next After 60 Years of G-Spot Debate? Other Possible Erogenous Zones in Female Genitalia Which Can Contribute to the Development of Female Orgasm Other than Glans Clitoris. The 34th NACS-Sexology Conference (Pleasure and Health) 4-7 October, 2012, Helsinki-Finland. NACS-Conference Abstract Book 2012; 34: 30-31. (c)
Sayin HÜ, Ramstadius M. Altered States of Consciousness (ASC) During Female Orgasms and Expanded Sexual Response (ESR): Don’t Use Drugs, Use Expanded Orgasms! The 34th NACS-Sexology Conference (Pleasure and Health) 4-7 October, 2012, Helsinki-Finland. NACS-Conference Abstract Book 2012; 34: 33. (d)
Sayin HÜ, Kocatürk A, Kocatürk C, Ramstadius M. Correlation of Factors that Contribute to the Masturbation Quality and the Strength of Pelvic Floor Muscles (PFM) as Measured by Kegel Perineometer. The 34th NACS-Sexology Conference (Pleasure and Health) 4-7 October, 2012, Helsinki-Finland. NACS-Conference Abstract Book 2012; 34: 32. (e)
Sayin HÜ, Kece C. Four Nerve and Six Pathway Theory of Female Orgasmic Response. The 34th NACS-Sexology Conference (Pleasure and Health) 4-7 October, 2012, Helsinki-Finland. NACS-Conference Abstract Book 2012; 34: 29. (f)
Sayin HÜ, Kocatürk A, Kece C, Dastan K. The Acute Effects of Nasal Oxytocin Spray on Female Behavior: Sedation, Arousal, Anxiolysis, Empathy and Altered States of Consciousness. The 34th NACS-Sexology Conference (Pleasure and Health) 4-7 October, 2012, Helsinki-Finland. NACS-Conference Abstract Book 2012; 34: 32. (g)
Sayin HÜ. Women and Orgasm: New Orgasm Theories in Sex Therapy (Kadın ve Orgazm: Cinsel Terapide Yeni Orgazm Teorileri). Ankara: Pusula Publications, 2013 (In press).
Schwartz L, Schwartz B. The One Hour Orgasm. New York: St. Martin’s Griffin, 1999.
Schiavi R C, Segraves R T. The biology of sexual function. Psychiat Clin
North Am 1995; 18: 7 –23.
Singer I. The goals of human sexuality. New York: W.W. Norton, 1973.
Stahl SM. The psychopharmacology of sex, Part 1: Neurotransmitters and the 3 phases of the human sexual response. Clin Psychiatry 2001; 62(2):80-1.
Sukel K. Sex on the brain: Orgasms unlock altered consciousness. New Scientist 2011; 2812. http://www.newscientist.com/article/mg21028124.600-sex-on-the-brain-orgasms-unlock-altered-consciousness.html?full=true.
Tannahill R. Sex in History, New York:Scharborough House, 1992.
Taylor P. PhD Thesis: An Observational and Comparative Study of Practitioners of Expanded Orgasm: An Investigation of an Effective and Accessible Path to Transcendent States of Consciousness, Submitted in Partial Fulfillment of the Requirements for the Degree of Philosophy in Transpersonal Psychology, International University of Professional Studies, Maui, Hawaii, 2000.
Taylor P. Expanded Orgasm: Soar to Ecstasy at your Lover's Every Touch, Illinois: Sourcebooks, Casablanca, 2002.
Vatsyayana, Kama Sutra, Trans. by Burton R., London: Private, 1883.
Weijmar Schults WC, van de Wiel HB, Klatter JA, Sturm BE, Nauta, J. Vaginal sensitivity to electric stimuli: theoretical and practical implications. Arch Sexual Behav 1989; 18: 87 –95.
Whipple B, Komisaruk BR. Analgesia produced in women by genital self-stimulation. J Sex Res 1988; 24:130-140.
Wolfe L. The Cosmo Report, London: Corgi Books, 1982.
Wu W and Humana C. Chinese Sex Secrets, New York: CFV Publications, 1996.
Zaviacic, M. The adult female prostata homologue and the male prostate gland: a comparative enzyme–histochemical study. Acta Histochem 1985; 77: 19 –31.
Zaviacic M, Dolezalova S, Holoman IK, Zaviacicova A, Mikulecky M, Valer Brazdil V. Concentrations of Fructose in Female Ejaculate and Urine: A Comparative Biochemical Study. J Sex Res 1988; 24: 319–25.
Zaviacic M, Whipple B. Update on the female prostate and the phenomenon of female ejaculation. J Sex Res 1993; 30: 148 –151.
Zaviacic M, Ablin RJ. The female prostate. J Nat Cancer Inst 1998; 90: 713.
Zdrok V. Anatomy of Pleasure. Philadelphia: Infinity Publishing Co., 2004.